What Is
Microtia
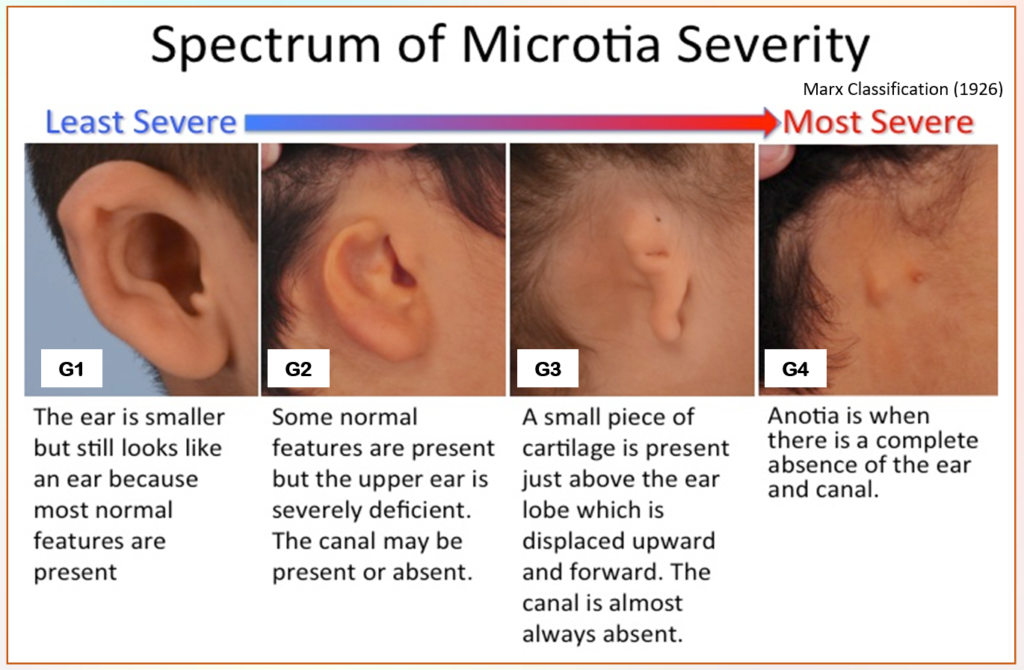
Microtia is a congenital condition in which the ear does not develop / develop properly during the first trimester of pregnancy.
The word Microtia translates to “small ear”.
Microtia occurs in every 6,000 to 12,000 births (* Hispanics *Asian * Native Americans * Andeans)
Dr. Sheryl Lewin, 2019
- (ratio) Boys : two times higher than Girls
- (ratio) Right ear – two times higher than Left ear
- Unilateral (1 small ear) Microtia >75%
- Bilateral (2 small ears) occurs <25%
- Microtia ears VARY in Shapes, Sizes and Grades
Syndromes associated with Microtia :
- Treacher-Collins Syndrome
- Hemifacial Microsomia
- Goldenhaar Syndrome
Other Conditions seen with Microtia :
- Spinal Anomalies
- Clefts
- Facial Asymmetry
- Kidney
- Heart
- Eyes
- Hand issues
Microtia Treatment Options
- Rib Cartilage
- Porous Implant (MEDPOR)
- Prosthetic
- No Treatment (unilateral)
Aural Atresia
Aural Atresia is an underdeveloped external ear canal, eardrum and middle ear bones.
- Aural Atresia is often associated with Microtia
- 90% with Microtia & Atresia have a conductive hearing loss
- Although the outer and middle ear anatomy is affected in Aural Atresia, most have a normal functioning inner ear (cochlea and auditory nerve)
Atresia Treatment Options
- Bone Anchored Hearing Systems
- Canalplasty
- No treatment
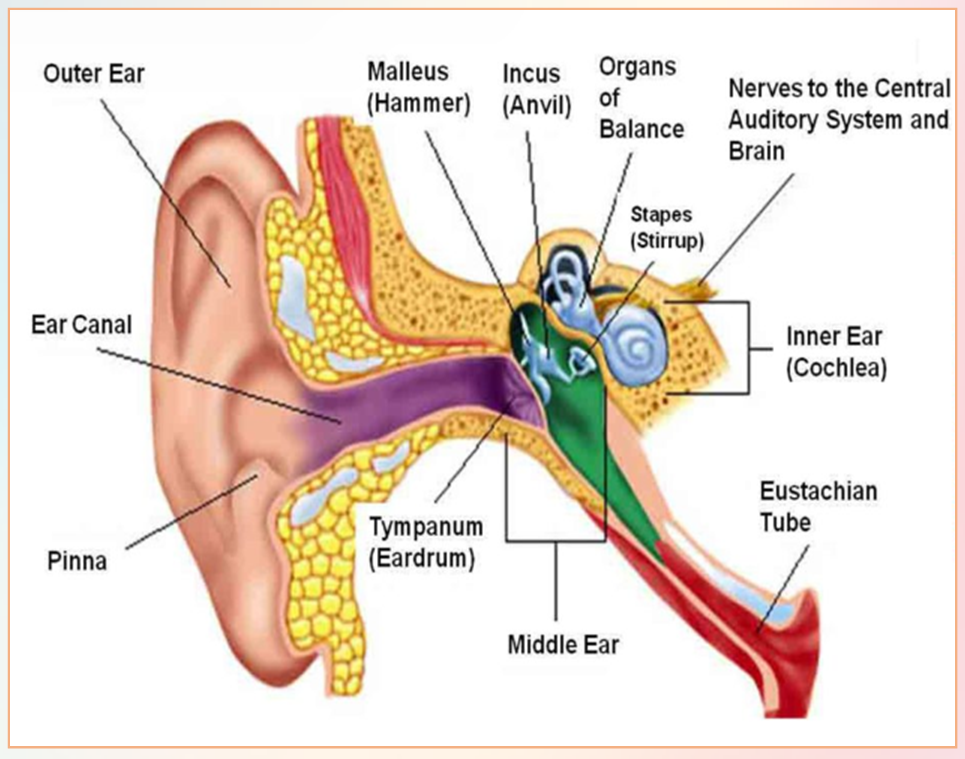
Structure of a Normal Ear
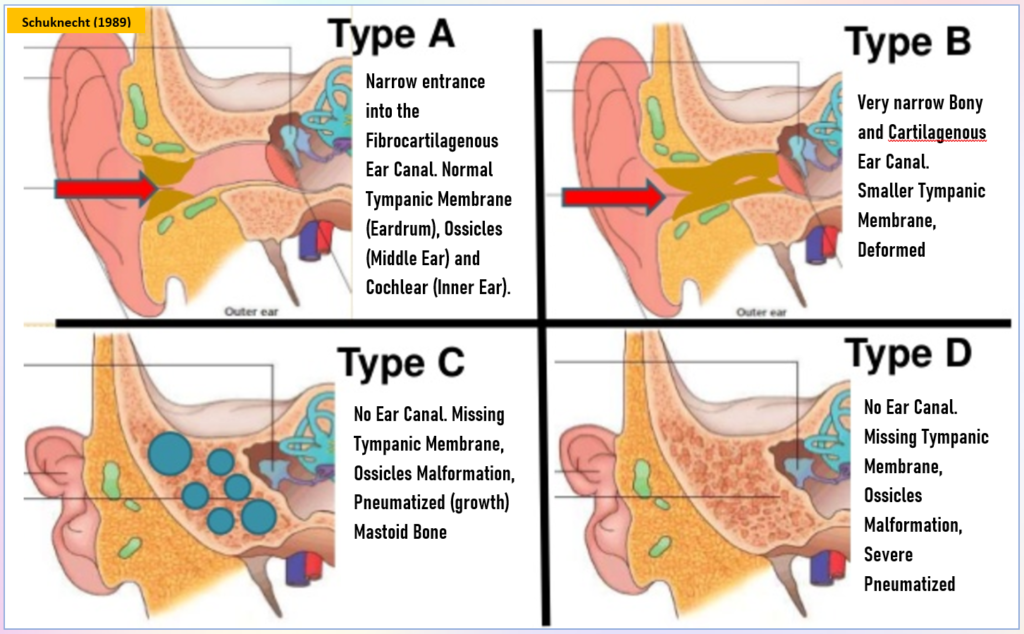
Schuknecht, 1989 describes 4 types of Aural Atresia :
Frequently Asked Questions
1. As a mother, did I do something during my pregnancy to cause my child’s ear(s) to be underdeveloped or missing?
No, there is nothing a mother did to cause Microtia and Atresia if you had a healthy pregnancy. There are too many variables to compare in women all over the world with their lifestyles (such as the food they ate, the water they drank, altitude lived in, overall general health, medication taken, allergies/colds, and how active they were during their pregnancies, etc…). Sometimes, things just happen in utero that are unexpected, even with the healthiest of pregnancies.
2. Is Microtia and Atresia genetically inherited?
There is solid – yet preliminary – evidence that genetics plays a role in some patients. However, the majority of families who have a child born with Microtia and Atresia cannot find anyone in their family who has previously had underdeveloped or missing ears.
3. If my child can have reconstructive surgery, can I give my child my own ear for surgery?
Unfortunately not. A donor ear from a parent or relative will not survive on someone else. The tissue from another donor would be considered a foreign body to the recipient’s body and the donor tissue would not survive. Reconstructive surgery for a newly reconstructed ear would involve your child’s own tissue and biological materials needed to reconstruct an ear.
4. When considering reconstructive surgery, how soon can my child have ear surgery?
Many things must be taken into consideration when making the decision to have reconstructive surgery for Microtia and Atresia repair. Depending on how young a child is can help determine which surgical technique can be considered. The grade or severity of Microtia and Atresia can also affect the surgical technique you decide on because of how many stages of surgery may be required to reconstruct the ear (or ears) by using that specific surgical technique. Also, if considering the rib graft surgical technique for example, the surgeon may want the rib cartilage to have reached a certain maturity so that it is strong enough to be used during surgery. It may also be the surgeon’s preference for beginning surgery at a specific age for the child because of wanting to make sure the child does not pick at or rub the newly reconstructed ear and can help be responsible during the healing process.
5. At what age will my child notice his/her ear or begin asking questions?
By age three, most children discover that their ear or ears may be different from others and begin asking questions.
6. Should I raise my child differently because of having Microtia and Atresia?
It is important to raise any child with confidence, love and respect for him/herself. A child who is born with Microtia and Atresia is no different from any other child. Get to know your child’s personality and see what they would prefer if they are interested in making changes to their ear(s) in the future or keeping their ear(s) just the way they are.
Extracted from The Microtia and Atresia Clinic at Vanderbilt University Medical Center Website
First Steps

When a child is born with Microtia and Atresia, families will have questions on what to do next, which medical professionals to see, and what options are currently available for Microtia and Atresia
Where do I Begin?
1. Newborn Hearing Screening:
After a child is born, before leaving the hospital, a newborn hearing screening should be conducted to detect if hearing loss is present. If hearing loss is detected, your child will “refer” on the screening. At this point, your paediatrician will suggest setting up an appointment with an ENT and an audiologist. The paediatrician may also want to conduct a renal ultrasound and check your child’s heart, as the ear, kidneys and heart develop at the same time, during the first trimester of pregnancy.
2. Scheduling an appointment with your Audiologist:
Call to schedule an appointment with your audiologist for an ABR hearing test to be conducted. An ABR (Auditory Brain Response) hearing test will measure electronic responses that will be recorded from the hearing nerves and brain of your child helping determine how much of a hearing loss your child has. This test will also verify what type of hearing test your child has. This test typically takes about two hours and can be easily conducted if your child is under the age of six months so they can sleep through the test. If your child will not sleep on his/her own, the medical centre can sedate your child for this test. In addition to the ABR test, your audiologist will also conduct other hearing tests such as:
- AEP (auditory evoked potential evaluations)
- ASSR (auditory steady state response evaluations)
- SAT (speech awareness threshold)
- VRA (visual reinforcement audiometry)
- DP (OAE) and the TE (OAE) which are both auto-acoustic evaluations
3. Scheduling an appointment with your ENT:
While most ENTs will know little about Microtia and Atresia, do call to schedule an appointment to have your child examined in general by your local ENT to discuss your child’s hearing loss and helpful options. Your ENT can also make some recommendations on who to see regarding a professional who specializes in Microtia and Atresia care. A CT scan by any professional is discouraged during the early years of age if solely to examine the temporal bone since the study will need to be repeated later in life when discussing surgical options.
4. Medical professionals and therapists to consider visiting with:
- Paediatric Otolaryngologist
- Paediatrician
- ENT- Otologist/Neurotologist
- Audiologist
- Craniofacial Surgeon
- Paediatric Oral Surgeon
- Geneticist
- Speech Therapist
Extracted from The Microtia and Atresia Clinic at Vanderbilt University Medical Center Website